
Introduction
And so strong was the love of cleanliness thus encouraged, that women often toiled to wash their own and their children's clothing, who had been compelled to sell their hair to purchase food to satisfy the cravings of hunger.— John Timms, Curiosities of London 1855
As late as the year 2000 Sally Sheard identified the paucity of interest, let alone research, into an important aspect of “sanitary reform'': the provision of public baths and wash-houses. She notes that most research on sanitary reform in nineteenth-century Britain has tended to focus on the construction of “large-scale waterworks and sewerage systems (63).” She doubtless here refers to the achievement of Sir Joseph Bazalgette (1819–91) the engineer behind the creation of London's sewer system. While these, she acknowledges, played a significant role in making “improvements to the condition of the nineteenth century urban environment” the role played by public baths and wash-houses in “public health activity despite recognition of its significance in disease-specific mortality studies” has been largely ignored (63). It is a view supported by Edward Gibson the writer of an earlier paper that focuses its attention on the “widespread and intensive agitation for improvement of the public health ... culminating in the Pubic Health Act of 1848” in which the role played by the movement for public baths and washhouses is a “little noticed aspect” (391).
Pre-Victorian Support for Therapeutic Bathing
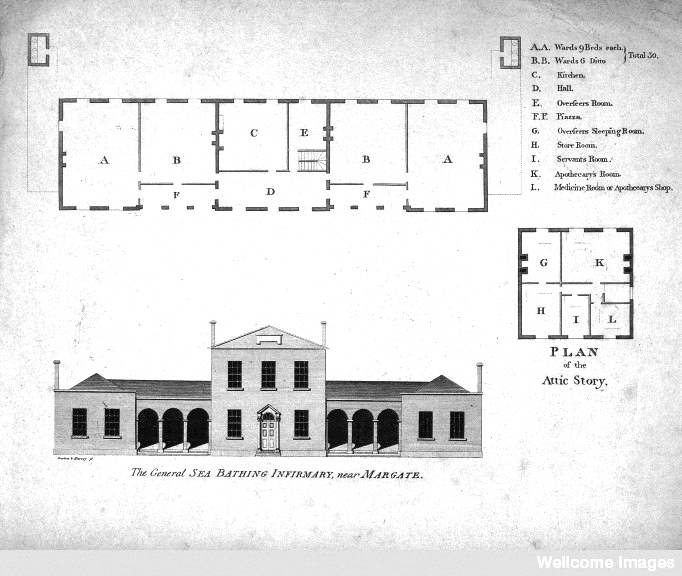
Left to right: (a) The General Sea-bathing Infirmary, Margate, Kent. Plan, c. 1800.. (b) Dr. John Coakley Lettsom. Stipple Engraving after W. Ridley, 1800, after S. Medley..
Gibson confirms that the English, prior to the 1840s, were by no means ignorant of the “therapeutic values” of bathing citing particularly the “quantity of literature on balneology published in England” before this period. He argues that “Most well to do people were convinced of the therapeutic values of the mineral waters of the British Isles. Bath [Somerset] was merely one of some 190 watering places to which the upper classes could repair. That the sick poor could also benefit the medicinal baths available ... seems to have been overlooked.”


Bath's Roman Baths and the Entrance to them
The “founding of The [General] Sea Bathing Infirmary at Westbrook in 1796, at which its director and other medical men supplied advice and medicines gratis to the poor, and a similar infirmary established at Margate soon afterward ... seem, however to be isolated examples” (392). Lauding this philanthropic institution, initiated by the indefatigable and generous Quaker physician John Coakley Lettsom (1744–1815)—and the therapeutic regimen of sea-air and sea-bathing it assured— one contributor to the Gentleman's Magazine (1816) wrote, that
whoever has any degree attended to the afflictions of their indigent fellow creatures in the Metropolis or its crowded environs, must have observed, with feelings of regret, how many have been dragging out a miserable existence from the dread effects of a most loathsome disease [scrofula],1 the debilitating nature of which is heightened by want of proper food, clothing, and cleanliness. [17]
The writer notes that “from its beginning to the present [1816] three thousand seven hundred and fifty-six patients have experienced ... the salutatory effects of this establishment,” most of whom had come from “the close and confined chamber of poverty and disease, situated either in some lane or alley of a populous city; several from the poor-houses of out-parishes, the hospitals and other charitable foundations” (17). Twenty years later little had changed.
The Turkish bath, its Supporters and Detractors
However, Sheard suggests that most public baths of the late eighteenth and early nineteenth century were seen primarily as cultural facilities rather than as a public health service. Baths had fallen out of favour for fear of venereal disease and by the stigma of “luxury” attached to them, and a perceived close association between baths and brothels (65, 66). The association of bathing with sexual licence is implicit in the very fabric of certain baths and bathing styles. This was particularly the case with the Turkish bath or Hamman. As a public bath the Turkish bath, or a form of it, had been introduced into England by returning Crusaders in the medieval period. Plague, which scared off the customers and “immoral business done on the side'', led to their demise (Wright 58-60). In the reign of Henry VIII public communal baths or “stews” were closed and remained so until “the late eighteenth century by which time few cared to be clean, and bathing was a curative rather than a cleansing process” (60). With medical support the Hamman again became fashionable in London in the mid 1850s, mainly through the efforts of diplomat and orientalist David Urquhart (1805–77) who created the exotic, private and masculine environment of the Jermyn Street Hamman in the fashionable West End of London in 1862 (Kandela "Rise and Fall" 70, 74; Potvin, 319, 320, 321).


Left to right: (a) The cooling room in the Turkish Baths in Jermyn-Street. (b) The hot-chamber. Illustrated London News 42 (26 July 1862): 96.
Turkish bath. n. 1. a type of bath in which the bather sweats freely in a room heated by hot dry air (or in a series of two or three rooms maintained at progressively higher temperatures), usually followed by a cold plunge, a full body wash and massage [''shampooing''], and a final period of relaxation in a cooling-room.
During the 1860s discussion of the therapeutic benefits or otherwise of different types of bath remained a “live debate” within the pages of The Lancet particularly with respect to Turkish baths (Kandela “Sketches” 601). “Enthusiasm ... was [often] tempered by a rather tetchy Editorial questioning the real benefits.” Rather than anecdote the editors wanted definite proof of the kind of disease that was relieved by the Turkish bath. Without facts to the contrary the editors considered taking a bath the English way was more appropriate for Englishmen:
There is a well-known institution of “tubbing” in cold water each morning, and of promoting the action of the skin and the renovation of the body by manly exercises in the open air, amongst which walking, cricketing, and rifle drilling are the simplest and most efficient . . . The time devoted to the bath would be better employed at the drill; and while tubbing flourishes Englishmen will not need to waste long hours daily on the effort to wash and to perspire. [601]
Indeed, toward the end of the nineteenth century Robert Owen Allsop, architect and author of The Turkish Bath: Its Design and Construction (1890), could still write that he hesitated “to employ the designation 'Turkish Bath,' because to do so seems immediately to create in many minds the idea of luxury pure and simple – coffee and cigars apparently, being more obvious than clean skin” (5).
The Public Bath and Washhouse as a focus for Victorian Social Reform
However, the question arises as to the extent to which public baths and washhouses improved the health of the wider public and particularly the poor who were to be the focus of so much attention by nineteenth century social reformers?
George Rosen (1910–77) in his A History of Public Health (1958) points out that as industrialisation advanced from the late eighteenth century onward more and more people lived in towns and worked in factories, and as this new way of life spread, health conditions deteriorated, leaving far behind any voluntary, piecemeal efforts to cope with the problem. Thus between 1800 and 1841, the population of London leaped from 958,000 to 1,948,000, that of Leeds expanded from 53,000 to 123,000, and that of Huddersfield, from 15,000 to 34,000. What this meant for the country is shown in Table 11, which gives the percentage of the population of England and Wales living in urban communities of various sizes from 1801 to 1861. This rapid growth was soon reflected in mounting death rates [and] the rapid growth of the urban population outpaced any increase in available housing. As towns shot up suddenly, the problem became one of packing in as many people as possible, as fast as possible, somewhere, somehow, anyhow ... [E]very bit of space was built on with the result that excessive densities became common features of urban communities (Rosen. 202).
Because of “financial considerations” Rosen continues, “there was virtually no planning” with manufacturers building factories where they needed them and speculative builders erecting poor quality housing on any land available in close proximity to those places of employment (203). This was exacerbated by the fact that there was “no real choice as far as residence was concerned” as much labour was of a casual nature and it was a matter of being (and living) on the spot or lose the opportunity of earning the pittance needed for subsistence (203); a way of life variously portrayed in the novels of Charles Dickens (1812–70) the etchings of Gustave Doré (1832–83); and in Henry Mayhew's (1812–87) London Labour and the London Poor (1851-72) a chronicle of the lives of those who “obtain[ed] their living in the streets of the metropolis” (5). It was a task later taken on by other social commentators, such as Charles Booth (1840–1916) in Life and Labour of the People of London (1903).2
The bathhouse and washhouse movement falls into this time frame and is as much the story of the reorganization of the state bureaucracy as it is of the (re) organization of the people who were served and affected by the apparatus of the state. The movement forms a modest but important part of a greater legislative program aimed at “improving” the conditions of the towns cities of England during the early to middle decades of the nineteenth century when, according to historian Asa Briggs, the “economic, social and political history of England seemed to be falling into shape” (2).
The Poor Law and Poor Law reform and its Consequence for Public Health
The first decades of the century were a time when successive administrations sought to create a new relationship between central and local government (Prest 14). In 1830, after “fifty years in the [political] wilderness” the Whigs under Lord Charles Grey (1764–1845) were returned to government. And, after introducing, and seeing passed, the Reform Act in 1832—which corrected long-standing abuses in the electoral process—they turned their attention to other legislation (14-25). Significantly they turned their attention to reform of the old poor law. Under the old poor law [1607] local parishes bore the responsibility of supporting their legally resident (born, in the parish) poor as well as defining poverty and setting the level and type of support given. “The result was a national system of relief characterized by diversity rather than uniformity” (Hanley 407). At the same time rapid industrialization population growth had put a severe strain on the cost of providing poor relief resulting in both a cost blow-out for government—poor relief climbing from £2,000,000 in 1784 to £8,000,000 in 1818 (£7,000,000 in 1832)— and an increasingly fractious population of impoverished people prone to riot; which, in 1830 they did, resulting in a number of hangings and transportations. Such was the fate of one young woman called Elizabeth Studham who burned down a workhouse in Margate and was transported for life to Van Diemen's Land [Tasmania] (Rosen Public Health 202-204; Rosen 431-41; Wilson 6).
In February 1832 the Government initiated the “Royal Commission for Enquiring into the Administration and Practical Operation of the Poor Laws.” The Commission had eight members including the economist Nassau William Senior (1790–1864) and Edwin Chadwick (1800–90)—a friend and associate of Jeremy Bentham (17481832)—first as an assistant and later as a full Commissioner. Chadwick, a barrister and journalist, had been made aware of the crowded disease-ridden slums of London through his association with two doctors: Thomas Southwood Smith (1788–1861) and Neil Arnott (1788–1874) both of whom had an interest in sanitary reform (Hamlin 17).
The new Poor Law that resulted from their efforts—''probably the most hated single law of the nineteenth century''—was governed by the principles of the “workhouse test” and “less eligibility.” An able-bodied man seeking poor relief had to seek it in the workhouse where “the condition of the pauper [had] been made less eligible” (that is, less attractive) “than that of an independent labourer offering his labour in 'a free and mobile'” labour market. There would be no other external support. The workhouse was a grim institution where families were deliberately separated in a regimented environment, which they could escape through work if they could get it (Briggs 280; Rosen 420; Wilson 14).
Chadwick admitted that his interest in sanitation grew “indirectly” out of this association with the Commission, when “some investigations with a view to discriminate the causes of pauperism, excessive sickness, and its preventable causes were presented in the course of the enquiry” (Finer 157). In 1838 he got permission to carry out a survey sending Arnott, Southwood Smith and James Kay (later Kay-Shuttleworth [1804–77]) together with a small team of assistants to investigate “the chief removable circumstances affecting the health of the poorer classes” (Chadwick 75).3 As Christopher Hamlin puts it, “they set out to discover the cause of fever in the East End ... and [found] it to be filth” (17). For Chadwick this was true: “He went to his grave still not believing that bacteria could cause disease” (Freyman 529). He would have agreed that “air ... is often charged with noxious exhalations arising from the putrefaction of animal and vegetable matter.” Nevertheless his attachment to miasmatical ideas particularly during these years of fever led directly to “massive sanitary reforms” and, it is argued, ultimately made the bacteriological basis of disease easier to accept (Tesh 1004, 1006–10).
The “Sanitary Idea”
In May 1842 Chadwick's Report on the Sanitary Condition of the Labouring Population of Great Britain and on The Means of Its Improvement appeared. It proved an immediate success. And, it led eventually to the Public Health Act of 1848. “A sign,” Asa Briggs argues “that the “Sanitary Idea” had established itself as a leading idea of the age.” Just as the new General Board of Health (1848) he suggests, “reflected the influence of the [new] Poor Law of 1834 on the structure of [public] administration.” Yet “outside the framework” of these laws and bureaucratic structures “important social measures still depended on the initiative of philanthropists” and others including “experts” and pressure groups to make things happen! (Briggs 335). And while the Board of Health was dissolved in 1854 the notion of government involvement in the health of the people remained; creating a new relationship between the individual and the state. As Mary Poovey notes:
Eventually, all this poor law information generated ... a new picture of an adjacent problem that needed to be surveyed, tabulated, legislated, and administered by representatives of the political domain. The problem of public health, which became visible as the poor rates increased in urban areas, directed official attention to poor neighbourhoods, which had been the object of concern for medical men since the early years of the decade ... The government-sponsored Sanitary Report of 1842 contributed to the project of cultural formation by extending the domain of the social and by specifying the relationship between its management and [other] domains. [12]
The Impetus for Change: The Bathhouse and Washhouse Movement in 1844
Thus, the result of the report was two-fold. It led to a greater awareness by government of urban social and infrastructure problems and to an increased support for action by “a large and growing body of public men, organized in a number of voluntary associations.”
The creation of this outdoor public opinion began in earnest in 1844, when a number of associations were formed, the Association for Promoting Cleanliness among the Poor, the Society for the Improvement of the Conditions of the Labouring Classes, and the Health of Towns Association. The first aimed to set up Baths and Wash-houses...(Finer 217).
Public baths were not generally available to the working class before 1842 (Gibson 392). People bathed (if they did) in the rivers or sea if they could. Some effort was made early on and public baths and washhouse were erected in Liverpool in 1828 (Allsop 2, 3). Birmingham had a complex of ten baths for both sexes in 1831 (Markus 151). But as with all innovations progress was slow and usually reactive stimulated by yet another outbreak of disease. There also remained another impediment to personal cleanliness. The Soap Tax levied in the early 1700s was still in force and only reduced in 1833 (Greene 205). In 1835 Mr J. Silk Buckingham introduced a Bill into the House of Commons, but it was rejected. On 8 June 1842 an anonymous writer from Mile End suggested to the Times that 290 acres of land granted by the Queen for a park between Regent's and George Duckett's Canal be the site for a bathing facility fed by the waters of the canal. Nothing came of this plan (Gibson 396).
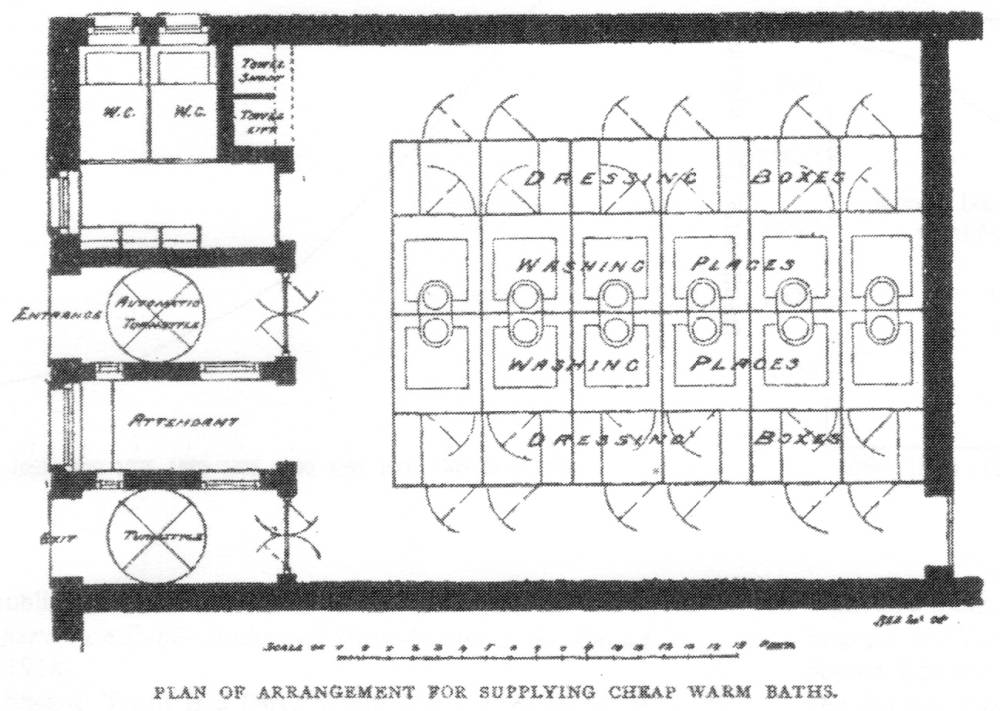
Baths for the Poor from Robert Owen Alsop, Public Baths and Wash-houses (London: E. & F. N. Spon, 1894), 86.
It was not until 1844 as a result of a Royal Commission into the Sanitary State of Large Towns and Populous Districts that there was movement. The commission identified the absence of cheap baths and a lack of public laundry facilities as an impediment to better health. This lack left the poor to clean themselves and their clothes as best they could within their own crowded houses (Sheard 66). Nevertheless, as recorded in the Times on 17 October 1847, it remained to some notable and public-spirited people to initiate action when (after an initial planning session on 14 October) at two o'clock on October 16 1844, “a public meeting was held in the Egyptian Hall of the civic Mansion House for the purpose of forming an association to furnish the labouring poor with baths and washhouses.” The newly formed Association for the Establishment of Baths and Washhouses for the Poor eventually “became known as the parent committee of the movement in London” (Gibson 396). It provided the encouragement and the funds needed to set up the first “experimental” public bathhouse in a renovated building in Glasshouse Yard, East Smithfield near the London Docks in 1845. In its first year 35,000 used it for baths and 49,000 for washing and ironing; by the end of June 1847 “the bathers, washers, and ironers amounted to 84,584; the bathers and washers costing about one penny each ... The association also gave whitewash, and lent pails and brushes, to those willing to cleanse their own wretched dwellings” (Markus 151). There had been scepticism and concern that the poor would not take advantage of the new service. But, as celebrated in the Times on 16 December 1845, the opposite was the case and the seven months” experiment
proved most incontestably, that the very lowest poor, those who have for years been habituated by hard necessity to the endurance of personal filth, and whom some might therefore regard as wholly indifferent to its continuance, will eagerly avail themselves of any facilities afforded to them for attaining personal cleanliness.
Petitions to the House of Lords for Increased Sanitary Facilities for the Masses
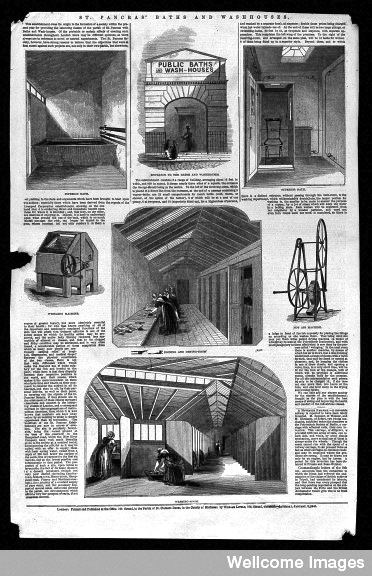

Left: Details of St. Pancras Baths and Washhouses. Wood Engraving, 1846.. Right: The later St. Pancras Public Baths and Public Hall designed by Thomas W. Aldwinckle. 1898-1900.
The Association promoted the building of London's first purpose built public bathhouse at St Pancras in 1845, one that was so successful that the Association began another more ambitious project in Goulston Square, Whitechapel. While, according to the popular magazine John Bull, 3,254 men and boys used the baths in its first week, Goulston Square did not flourish until it was later taken over by the Vestry of Whitechapel.4 A private bathhouse for the poor was built in George Street, Euston Square in 1846 with water supplied by the New River Water Company. The water company subsequently closed its reservoir and the bathhouse was forced to close (Allsop 3; Markus 151). It was evident that “public baths and washhouses would not flourish under [either] semi-philanthropic or private enterprise. Public measures were required” (Allsop 4). Thus, on 8 June 1846, the Bishop of London and former poor law commissioner Sir Charles James Blomfield (1786–1857), “presented five petitions ... to the House of Lords, praying for increased facilities for cleanliness available for the masses, and on the 19th of the same month, Sir George Grey introduced the Bill into the House of Commons. There was no opposition in the House and the Bill passed without debate on 24 July 1846 (4). The Bill was passed in the House of Lords on 7 August 1846 and received Royal assent on the 26 of August, 1846.” The Act (which was “permissive” or non-binding)5 to establish the Public Baths and Washhouses for the first time “enabled parishes and town councils to build public facilities, meeting the construction costs out of the Poor Rate and repaying this within a fixed term.”


Left to right: (a) The Wells and Camden Wash Houses and Baths (1888) (b) Camberwell Public Baths (1890-91).
Private enterprise would be encouraged to build baths while corporations and vestries would make these “on the one hand accessible to the poor, and on the other hand remunerative to the town or parish in which they were established” (Sheard 67). The baths would also, it was hoped, be self-supporting and would ultimately be of benefit to everyone. To this end the following year the Act was amended to allow for an increase in charges to be levied for superior facilities for those who were willing to pay (67; Gibson 406). The first metropolitan bathhouse to be built under the new Act of 1847 was that of The Baths and Laundries of St. Martin's in the Fields which made use of what had been learned in establishing and constructing the baths at the Public Model Baths at Goulston Square (Price 172–75). Other baths and laundries followed and six years later the Times sang the praises of the movement; the Committee providing the statistics to prove the success of the enterprise. It was proof not only of the wisdom of those behind the legislation but “pleasing proof of advancing civilisation” as well:
Our ancestors did not trouble themselves, either medically or morally, about such matters [cleanliness and physical comfort]; but happily modern ideas run in a directly opposite channel. Our doctors have taught us that if we would avoid epidemics, or at least deprive them of their full virulence, we must above all things avoid dirt—dirt in any of its countless forms. There may be dirt in the air, dirt in the water, dirt in the sewer, dirt in the floors and walls of our dwelling-houses, dirt on the clothes, dirt on the skin. We must get rid of it all, if we are chary of our own safety and comfort ... if we care for length of days, free from suffering and discomfort, we must wash and be whole.
The continuing tax on soap had made it difficult for the poor to take full advantage of the new baths and washhouses. “A Friend to Cleanliness” bemoaned this fact in a letter to the Editor of the Times, 4 February 1845: “when the active exertions of the philanthropic are constructing baths and washhouses for the poor, surely it is fitting that so important an article in cleanliness as soap should be put within their reach as cheap as possible.” The Soap Tax was eliminated in 1853. However, fancy facilities were not necessary. “A rough towel and a lump of soap are more accessible medicaments with the great mass of mankind.''
Evidence for the Benefits of Public baths and Washhouses for the Poor
To what extent was “length of days, free from suffering” increased for the folk newly benefiting by this seeming revolution in cleanliness? Is the bathhouse and washhouse movement implicated in the decline in mortality that epidemiological statistics suggest occurred in Britain during second half of the nineteenth century? (McKeown and Record Gibson does not speculate on this, however he does say that while the movement “proved immediately popular” and “persisted in pubic favour for many years,” it did so “while sewerage, drainage, water supply and housing ... were to remain unsolved problems in the metropolis and ... most populous manufacturing towns” (Gibson 406). Sheard notes that the early phase of movement, during the 1840s, 1850s and 1860s, was “often a direct response to a perceived threat from infectious epidemic disease,” the focus changed during the century to reflect “a changing disease panorama” and
a subjective reassessment of the benefits that could be gained by, first, providing public facilities, and secondly, placing them within the means of the poorer classes both geographically and financially. Underpinning changing attitudes to the need for public baths and washhouses was an ongoing discourse suggesting that the working classes themselves were reluctant to use them because their opening hours were limited, they were far from their homes, and they cost too much. [75]
Sheard also makes reference to the “chronic water supply problems” which often stymied development but which many city administrations tried to overcome if they could do it cost-effectively. It was often left to private initiative to act (69). The whole history of the bath and washhouse movement is a demonstration of this tension between public and private action and public and private values.
Thus Liverpool incorporated public baths and washhouses into its early programmes for sanitary reform in the 1840s and 1850s. Yet the impetus was lost and the shift in perception of public baths from a sanitary to a recreational function legitimised the [Liverpool] Corporation's transformation of the service into a municipal trading activity, governed primarily by profit (77).6
Well into the twentieth century public baths and washhouses were perceived, somewhat, as a “secondary sanitary system,” with patchy development and continual concerns regarding cost to ratepayers and the fee-structure for those most in need of such facilities. In what was a gradual process, between 1845 and 1915, 345 public baths and 69 washhouses were been built in Britain, all maintained by a public authority, with most towns over 50,000 having some form of bathing facility (Campbell 8, 9; Sheard 68).
Gibson wrote in the period just before the historical analyses of medical historian Thomas Mckeown (1912–88) became prominent. Briefly, McKeown argued that the decrease in mortality and “the modern rise of population,” that occurred in the industrialised world from the 1700s to the twentieth century was the result not of clinical medical advances or public health initiatives but due to overall “improved living standards, notably rising nutrition” (Colgrove 725, 726; Szreter 427, 428).7 His historical analysis called into question the effectiveness of some of the most basic and widely applied techniques in the public health armamentarium, including sanitary reforms, vaccination, and quarantine ... and shaped the research hypotheses of many scholars and became the subject of extended controversy (Colgrove 725).
A graph showing an increase in bathhouse and washhouse facilities built between 1850 and 1915 (the time-frame which is the focus of McKeown's analysis) and a graph showing a decrease in mortality for infectious disease, while simplistic, does support the idea that at least some sanitary advances were implicated in a decline in mortality rates at least for adults (Sheard 68; Kass 111).
An increase in bathhouse and washhouse facilities built and a decrease in mortality for infectious and other diseases “correlated roughly with improving socio-economic circumstances” (Kass 111). Attempts to deal with the mid-century overcrowding that had “driven thousands of 'troglodytes' and 'human moles' to live in underground cellar rooms” was such an effort (Wohl 3). As were all attempts to create a better-built environment, such as slum clearance and Bazalgette's sewerage system—begun only after “The Great Stink” (1858) in 1859—carried out over time. Edward Kass gives the useful example (although it is for a later date) that “rates of rheumatic heart disease were almost linearly related to crowding in the home” and that “similar data gathered during World War 1 ... showed that when beds in barracks were placed too close together rates of meningococcal infection among troops rose abruptly” (111).
Those who were close in time to the sanitary improvement(s) being made, and that included the building of the first bathhouse and washhouse facilities, considered that the
decline in mortality was quite definitely causally linked to the burgeoning programmes of sanitary reform and the concentrated sanitary efforts of local government ... and were clearly aware of the major strides which had been taken in the direction of a more regulated and healthy environment by the developments in science, preventative medicine and sanitary engineering (Bell and Millward 225).
It was however a very long, drawn out, complex, and often frustrating (and unfinished) process on all levels, as a reading of Henry Jephson's The Sanitary Evolution of London (1907) reveals. He lauds with a degree of cynicism the “sudden display of Parliamentary energy” when in 1846 it decided to establish baths and washhouses for the poor. Only to make the Act “purely permissive or facilitatory''! (Jephson 39). A situation that remained [1907] and would not improve, he argued, until there was central, Parliamentary control (and compulsion) in all matters relating to public health (431, 432).
Negotiated Reform: Reform Through the Action of Government and People
Simon Szreter, in a partial critique of the Mckeown thesis, argues that the noticeable decline in mortality that the aggregate statistics reveal as beginning in the 1870s “was due more to the eventual successes of the politically and ideologically negotiated movement for public health than to any other positively identifiable factor” and that “the resulting implementation of preventive measures of municipal sanitation and regulation of the urban environment actually arrived on the ground” by the end of the century and beginning of the twentieth century. And this came about, he argues, “not through some “invisible hand” of rising living standards, conceived as an impersonal and ultimately inevitable by-product of general economic growth” but through the actions of “those agencies [local government and parochial] which brought about the implementation of these preventive health measures throughout the length and breadth of the land” (5, 26, 34, 35).
The agitation for what Gibson referred to as a “prosaic but useful service” was championed and carried along by many individuals and small associations (406). Often acting from a personal conviction that they were bettering the lot of their fellow citizens and in doing so improving the society they all shared. Whether writing a concerned letter to the Times or attending a meeting at the Mansion House they all knew that the bathhouse and washhouse movement represented an idea whose time had come.
Created 3 May 2013
Last modified 24 March 2023