
This article has been peer-reviewed under the direction of Professors Mary Elizabeth Leighton and Lisa Surridge (University of Victoria). It forms part of the Great Expectations Pregnancy Project, funded by the Social Sciences and Humanities Research Council of Canada.
In 1895 Arabella Kenealy, a eugenicist and retired doctor, wrote a letter to the British Medical Journal recounting a house call that she had supposedly made a few weeks earlier. The “wreck of a young woman” whom she attended was bleeding heavily and on the verge of miscarriage (682). Learning of her patient’s experiences — three miscarriages, a child with a characteristic congenital taint and a further two miscarriages — Kenealy’s diagnosis was swift: syphilis. Initially sympathetic, she tore up her prescription upon seeing the sole living child, whom she scorned as “so monstrous a ‘degenerate’” (682). Withholding treatment would likely lead to miscarriage, but in Kenealy’s mind this was the only acceptable outcome. She believed that in the mother’s womb grew a similarly diseased child that “Nature, abhorrent, was striving to cast off” (682). Kenealy’s account of wrecked womanhood and hereditary degeneration was heavily infused with the type of melodrama more commonly associated at the time with the work of New Woman novelists (among whom she counted herself). But it also highlights a number of serious challenges and anxieties in the care of pregnant women and unborn children.
Jonathan Hutchinson, photographed by Barraud. Courtesy of the Wellcome Collection. Attribution 4.0 International (CC BY 4.0).
At the best of times, pregnancy in the nineteenth century was a danger to mothers and their babies. It was substantially more dangerous for women infected with venereal diseases (VD), which to Victorian doctors meant either gonorrhoea or syphilis. Also evident was the terrible impact of VD on reproductive health. Afflicted women might be unable to conceive, or they might conceive and then miscarry or give birth to still-born babies. On the other hand, VD could cause terrible suffering for children living with conditions like gonorrhoeal ophthalmia neonatorum (a form of neonatal conjunctivitis) or congenital syphilis (Hanley, “Scientific Truth,” 200–01). Less certain were the modes of transmission or “inheritance.” Similarly, the diverse and inconsistent ways that VD manifested seriously hampered attempts at diagnosis. Many women infected with gonorrhoea were asymptomatic or presented with mild symptoms that might have been caused by a range of other conditions. Likewise, syphilis, described as “an imitator” by Jonathan Hutchinson (1828–1913), often produced symptoms (such as sores, rashes, vaginal discharge, ocular atrophy and neurological dysfunction) that might easily be caused by a variety of other conditions (“An Address on Syphilis” 499). Scientific breakthroughs came with the identification of the gonococcus in 1879 and the spirochete in 1905, as well as the development of new diagnostic technologies such as Gram staining (a method of staining to identify different forms of bacteria, such as gonorrhoea) and the Wassermann reaction (a blood test for syphilis). But even with these tools at hand, real change came slowly. Diagnoses continued to rely on the observation of physical symptoms. Yet many doctors were not adequately trained or sufficiently experienced to recognise women’s symptoms as gonorrhoeal or syphilitic (Hanley, Medicine, 28–30).
Gonorrhoea
Writing in 1889, Charles Cullingworth, consultant to St Thomas’s Hospital, London, lamented that “there is little doubt that, although gonorrhoea in the female is still regarded in this country as a comparatively unimportant affection, it really destroys the health of a larger number of women than does the poison of syphilis” (Cullingworth 122). Even into the Edwardian period, many doctors lacked the gynaecological knowledge and experience to comprehend the true prevalence and severity of gonorrhoea in their female patients. Early symptoms might go unnoticed or be misattributed, with the disease passing into an acute stage with the onset of menstruation or pregnancy. Indeed, in 1914 David Watson, surgeon to the Glasgow Lock Hospital, argued that pregnancy was a catalysing factor that furnished gonorrhoea with “the conditions which favour its growth, the symptoms are more marked, exacerbations more frequent, and complications more liable to supervene” (Watson 282). Having spread to the uterus, fallopian tubes, ovaries or peritoneum, gonorrhoea would often produce pelvic inflammation and pain, vaginal discharge, endometritis (inflammation of the lining of the uterus), salpingitis, painful urination and menorrhagia (a collection of symptoms now classified as pelvic inflammatory disease).
The exacerbation of gonorrhoeal infection could destroy a woman’s reproductive health, rendering her infertile. Yet large numbers of infants were developing ophthalmia neonatorum after being infected by their mothers at birth. Consequently, some doctors, such as George Granville Bantock, Senior Surgeon to the Samaritan Free Hospital, expressed doubts about whether gonorrhoea could prevent women from falling pregnant (Bantock 749–51). Historians are looking increasingly at the historical impact of VD on fertility. But as Simon Szreter notes, a lack of clear historical data has made such studies exceptionally difficult (Szreter 3–4).
Syphilis
Women with VD without clear signs of infection might give birth to sickly children. Equally, many women with clear symptoms might give birth to healthy children. The complex and inconsistent effects of VD on fertility and pregnancy created problems for doctors trying to treat expectant mothers, prevent miscarriages and protect the health of newborns. These challenges were nowhere more acute than in the prevention and treatment of congenital syphilis. Unlike gonorrhoea, syphilis did not directly prevent conception. Rather, it might lead to antenatal and neonatal morbidity and mortality.
But not all women whose reproductive health was compromised by syphilis might demonstrate other clear signs of infection. In such cases, doctors might rely on a distinctive pattern of diminution in the severity of antenatal and neonatal complications, known as Kassowitz’s Law. Writing in 1887, Hutchinson, one of Victorian Britain’s leading authorities on VD, noted that “the inheritance of syphilis, when continued through a family of children, shows a tendency to fall off, and decreases in severity in each successive child, until it comes finally to an end” (Syphilis 70). A woman might miscarry several times, then give birth to one or more still-born babies. Later children might die within the first few weeks of life or live into adolescence or adulthood with congenital syphilis. Eventually, she might give birth to children who showed no signs of infection. Hutchinson recounted a tragic case where the wife of a fellow doctor had seemingly escaped infection from her husband but demonstrated a clear pattern of syphilitic infertility. She experienced two still-births and had then given birth to another two children who died in infancy. Her next seven children lived, but each had congenital syphilis. Hutchinson concluded that “it would appear that eleven conceptions have in succession been tainted” (Syphilis 427). This principle of diminution was still being used in the early twentieth century because it enabled doctors to determine, in the absence of other clear indicators, whether their female patients were syphilitic (Royal Commission, q. 11767, 397–98).
The difficulty of establishing whether a woman was syphilitic was not the only challenge confronting doctors in their efforts to understand how syphilis was transmitted in pregnancy and how it might be prevented. Modes of congenital transmission remained a subject of speculation throughout the nineteenth century. Doctors like Hutchinson believed that congenital transmission in the mother’s uterus occurred when the syphilitic “virus” passed directly from the parent’s “fluids” to those of the foetus (Syphilis 64–65). But, according to these doctors, the precise mode of this transmission might vary: “It may be that it is from the father alone, or from the mother alone, the poison being in each instance present in the one parent at the time of their child’s conception. To these modes we may give the name ‘conception inheritance,’ qualified as ‘paternal’ or ‘maternal,’ or ‘sperm inheritance’ and ‘germ inheritance’ respectively” (Syphilis 65). Although “sperm inheritance” was thought to be the only possible mode of direct paternal transmission, it was believed that syphilis might be communicated from the mother in a variety of ways. A woman who conceived when already syphilitic might infect her unborn child through “germ inheritance.” Alternatively, a woman who was free of infection at the time of conception but acquired syphilis during pregnancy might infect her unborn child through the “placental circulation” of tainted blood. And because there were nine long months during which the foetus might be exposed to such risk, Hutchinson concluded that it had “much less chance of escape if the mother be diseased than if the disease be confined to the father” (Syphilis 65–66). Underpinning this belief was the implicit assumption that women were the principal vectors or reservoirs of contagion. As historians have noted, it was an assumption that also underpinned deeply flawed legislation like the Contagious Diseases Acts and similar colonial ordinances that were intended—but inevitably failed—to curtail the spread of VD.
Nineteenth-century doctors may have asserted the importance of swift and thorough treatment, but they were increasingly aware that available treatments had limited therapeutic effect and were often messy, protracted and the cause of much distress. The medical establishment continued to rely on these treatments because there were no satisfactory alternatives until the development of salvarsan and its substitutes in the 1910s, sulphonamides in the 1930s, and, eventually, penicillin in the 1940s (Hanley, Medicine, 110–25).
Doctors recognised that mercury—the most common treatment for syphilis—needed to be administered with the utmost care. This was even more imperative when treating pregnant women. Although Kenealy refused to prescribe mercury in the hope of inducing a miscarriage, other doctors refused to treat pregnant women with mercury precisely because it might have harmful effects on foetal development and even induce miscarriages. But here again professional opinion was split. The celebrated French venereologist Alfred Fournier (1832–1914) insisted that mercury would only produce such negative results if “ill-administered” (such as too frequently or in overly concentrated doses; Fournier 189). For him, “the skilled and prudent administration of mercury … appropriate to the constitution and special conditions of the patient” represented the “best and surest means possible of bringing pregnancy to a satisfactory conclusion and protecting the foetus” (189). Although conceding that women often miscarried during or after a course of mercury, he attributed this to the disease itself, asserting that “syphilis constitutes one of the most powerful predispositions to miscarriage” (192).
Eugenics, “Race Motherhood,” and Degeneration
Throughout the final decades of the nineteenth century, Victorian society was increasingly preoccupied with the threat of “degeneration”—a phenomenon bound up with eugenic ideas of racial and national fitness. Syphilis and gonorrhoea were just two among a wide variety of possible triggers for degeneration. But their terrible impact on fertility and the health of children made them particularly troubling, especially because they were also bound up with supposed moral decline. Writing in the Eugenics Review in 1909, the neurologist A.F. Tredgold (1870–1952) insisted that “the danger lies in the fact that these degenerates mate with the healthy members of the community and thereby constantly drag fresh blood into the vortex of disease and lower the general vigour of the nation” (Tredgold 102). Children born with congenital syphilis or blinded by gonorrhoeal ophthalmia neonatorum were viewed as the literal embodiment of this depleted national vigour.
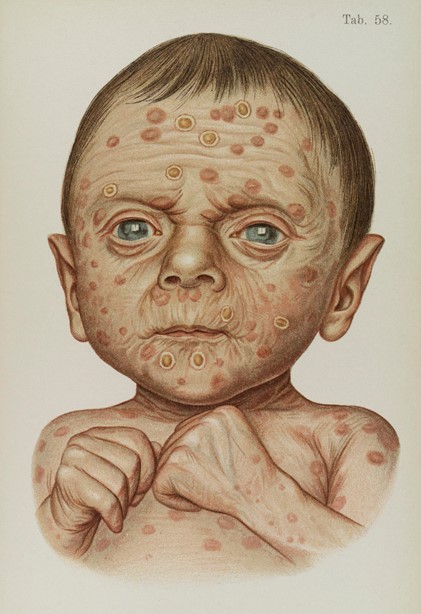
Illustration of baby diseased with hereditary syphilis. Courtesy of the Wellcome Collection. Attribution 4.0 International (CC BY 4.0).
Of the two diseases, syphilis was viewed as the most dangerous to the future health of the race and nation because it was believed to be hereditary—a view reasserted in the report of the 1904 Interdepartmental Committee on Physical Deterioration. Indeed, the suffragette Christabel Pankhurst shared this view, quoting C. F. Marshall’s description of syphilis as “the hereditary disease par excellence” in her 1913 critique of the social impacts of VD, The Great Scourge and How to End It (Pankhurst 72). For the Victorians, such degeneration was epitomised by the syphilitic child, who, soon after birth, would begin to display the characteristic signs of congenital infection, such as “snuffles” (inflammation of the mucous membrane of the nose), condylomata (genital warts), mucous patches, jaundice, and a characteristic coppery rash. Children so afflicted were often described in medical and popular literature as looking like old men, displaying what Hutchinson characterised as a “wasting and withered aspect” (Syphilis 74). As they grew, these children might develop Hutchinson’s triad of congenital syphilis—interstitial keratitis (inflammation and scarring of the cornea), notched teeth, and deafness—along with a range of other developmental complications. Such syphilitic symptoms were terrifying for a society preoccupied with eugenic notions of (un)fitness, the hereditary perpetuation of such malaise, and its associated burden on the state. Compared to the supposed threat of hereditary degeneration, health authorities paid little attention to infertility resulting from VD. For eugenicists like Kenealy, childlessness and the trauma of miscarriage were preferable to the birth of sickly children because it precluded the possibility of hereditary degeneration and its supposed associated decline of national and racial fitness.
Linked to this anxiety was increasingly vocal criticism of the sexual double standard and moral hypocrisy — the Victorian “conspiracy of silence” — that equated a woman’s innocence and respectability with her ignorance on all matters concerning sexual health (see Hanley, “I Caught It”). By the end of the nineteenth century, in large part through the efforts of the New Woman Movement, blame for the spread of VD was shifting away from working-class women. Instead, it was falling upon the sexual excesses of men and their exploitation of women. By denying women—viewed at the time as the moral and biological guardians of the race—the knowledge to choose a morally and eugenically “fit” mate who was free from physical and moral taint, Victorian society had become complicit in its own decay (Robb 58–59).
Bibliography
Bantock, George Granville. "On the Importance of Gonorrhoea as a Cause of Inflammation of the Pelvic Organs.” British Medical Journal (4 April 1891): 749–51. PMC (U.S. National Institutes of Health's National Library of Medicine). Web. 3 February 2022.
Cullingworth, Charles. "The Etiological Importance of Gonorrhoea in Relation to Some of the More Common Diseases of Women.” British Medical Journal (20 July 1889): 122–25. PMC (U.S. National Institutes of Health's National Library of Medicine). Web. 3 February 2022.
Fournier, Alfred. Syphilis and Marriage. Translation by Alfred Lingard. London: David Bogue, 1881. Wellcome Collection. Web. 3 February 2022.
Hanley, Anne. “‘Scientific Truth into Homely Language’: The Training and Practice of Midwives in Ophthalmia Neonatorum, 1895–1914.” Social History of Medicine (2014): 199–220.
____. Medicine, Knowledge and Venereal Diseases in England, 1886–1916. London: Palgrave Macmillan, 2017.
____. “‘I Caught It and Yours Truly Was Very Sorry for Himself”: Mapping the Emotional Worlds of British VD Patients.” In Patient Voices in Britain, 1840–1948, edited by Anne Hanley and Jessica Meyer, 299–337. Manchester: Manchester University Press, 2021.
Hutchinson, Jonathan. "An Address on Syphilis as an Imitator.” British Medical Journal (5 April 1879): 499–501. PMC (U.S. National Institutes of Health's National Library of Medicine). Web. 3 February 2022.
____. Syphilis. London: Cassell, 1887. Wellcome Collection. Web. 3 February 2022.
Interdepartmental Committee on Physical Deterioration. 1904, Cd. 2175. Wellcome Collection. Web. 3 February 2022.
Kenealy, Arabella. "A Question of Conscience.” British Medical Journal (14 September 1895): 682. PMC (U.S. National Institutes of Health's National Library of Medicine). Web. 3 February 2022.
Pankhurst, Christabel. The Great Scourge and How to End It. London: E. Pankhurst, 1913. Wellcome Collection. Web. 3 February 2022.
Robb, George. “Race Motherhood Moral Eugenics vs Progressive Eugenics, 1880–1920.” In Maternal Instincts: Visions of Motherhood and Sexuality in Britain, 1875–1925, edited by Claudia Nelson and Ann Sumner Holmes, 58–74. London: Palgrave, 1997.
Royal Commission on Venereal Diseases, 1914, Cd. 7475. (Appendix to First Report of the Commissioners, Minutes of Evidence). Wellcome Collection. Web. 3 February 2022.
Szreter, Simon, ed. The Hidden Affliction: Sexually Transmitted Infections and Infertility in History. Rochester: University of Rochester Press, 2019.
Tredgold, A.F. "The Feeble Minded: A Social Danger.” Eugenics Review (April 1909–January 1910): 97–104. PMC (U.S. National Institutes of Health's National Library of Medicine). Web. 3 February 2022.
Watson, David. Gonorrhoea and Its Complications in the Male and Female. London: Henry Kimpton, 1914. Hathi Trust, from a copy in the library of Columbia University. Web. 3 February 2022.
Created 3 February 2022